
First performed by Robert Rutledge in September 1997. Mini Gastric Bypass is a modification of Billroth II procedure, initially done for stomach cancers. Now, nearly 20 years and many more than 30,000 procedures later, a recent survey showed that the Mini Gastric Bypass appears to be growing into one of the top 3-4 bariatric and metabolic procedures in many countries around the world.
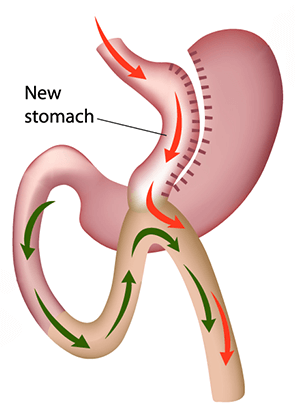
Long gastric tube and a wide loop anastomosis, to create a mal-absorptive and dumping effect.
The position of patient in the operation theatre is same as that in the Roux-en Y Gastric Bypass
Mini Gastric bypass is considered as a malabsorptive procedure where in there is less absorption of the consumed food.
There are similar 3 to 4 incisions or holes
In this the Gastric pouch is long, like a sleeve which is joined to the intestines, making a loop thereby finishing the procedure with only single anastomosis or joint.
The intestines that are bypassed are about 170 cm to 250 cm long depending on the requirement for each patient.
The results of excess weight loss and resolution of co morbidities is similar to that of RYGB.
It has a theoretical advantage over RYGB in reduced chances of intestinal obstruction in long term follow up.
The patient has a better capacity and tolerance to quantity of the food but as it causes more malabsorption the frequency of stools may be increased.
Post MGB, we have seen brilliant results in special subtype of our population.
